Sleeve Gastrectomy
How is the procedure performed?
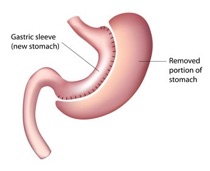
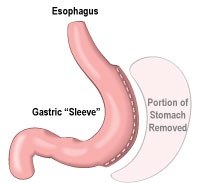
As with all other bariatric operations that we offer, Sleeve Gastrectomy Surgery is also performed laparoscopically (keyhole surgery). Small incisions are created in the abdominal wall to allow small instruments to be passed into the abdominal cavity, guided by a special surgical telescope with a video camera, in order to perform the operation. Sleeve Gastrectomy involves converting the stomach into a long thin tube. This is done by stapling the stomach along its entire length and then removing of approximately 75% of it.
How does the Sleeve Gastrectomy work?
This operation reduces the capacity of the stomach and thus restricting the amount of food that can be eaten. It also significantly lowers the level of the hunger hormone, ghrelin (a hormone produced by the parietal cells in the stomach) with the added benefit of reduction in hunger sensation and excellent weight loss.
How long will I stay in hospital?
Most people are discharged home the following evening. Some will stay an additional night or perhaps two depending on their health issues, especially their mobility, and availability of support at home. Our price package guarantee and 30-day insurance will cover the cost of any additional fees should your hospital stay after surgery need to be extended for whatever reason.
Who is suitable for Sleeve Gastrectomy?
The Sleeve Gastrectomy is a suitable option for most patients seeking weight loss. In particular, it is preferred over the gastric bypass in some special scenarios such as in those who have had multiple abdominal operations and/or complex abdominal hernia surgery with the placement of a mesh that could have resulted in extensive adhesions within the abdomen involving the intestine and rendering the gastric bypass rather hazardous due to risk of injury to the bowel and the likelihood for a longer operating time with added risk.
It is also a good choice for people who suffer with inflammation of the bowel such as ulcerative colitis and those who have coeliac disease (gluten allergy). Although acid reflux might well improve with weight loss, it is likely that it might worsen after a Sleeve Gastrectomy especially in individuals with severe pre-existing symptoms, and for such individuals the gastric bypass is a better option.
The chance of resolution of diabetes with the Sleeve Gastrectomy is somewhat inferior to that of a gastric bypass (60-65% compared with 80-85% on average); the bypass therefore is a better option particularly in people who have had diabetes for more than 5-10 years and who require multiple drugs and perhaps insulin to treat it.
How much weight will I lose?
The amount of the weight loss achievable with this procedure at 2-3 years is favourably comparable with the gastric bypass (on average, approximately 60-70% of the excess weight is initially lost).
What are the other benefits of Sleeve Gastrectomy?
In addition to weight loss, the Sleeve Gastrectomy has the following benefits :
Marked improvement or resolution in health conditions related to obesity, such as type-2 diabetes (approximately 60-65% chance of resolution), hypertension, gastro-oesophageal reflux, obstructive sleep apnoea, asthma, liver disease, high cholesterol, and painful osteoarthritis. Improvement in overall physical and psychological health Compared to gastric bypass surgery, the Sleeve Gastrectomy is a quicker procedure (25-40 minutes) as there is no cutting of bowel with less risk of nutritional complications. Also Dumping syndrome is unusual.
What are the risks?
As with any surgical operations there are associated short and long-term complications such as internal bleeding, leak, blood clot in the legs (deep vein thrombosis or DVT), blood clot in the lung (pulmonary embolism), infection, and weight regain.
Although the World’s literature quotes a risk of leak from the gastric tube of 1-5% and a risk of mortality of 0.5%, Dr Decadt has performed approximately 500 procedures to date with no leaks and 0.19% mortality. The stomach is tested at the end of surgery with a blue dye to ensure “no leak”, but until it has fully healed (which takes 2-3 weeks) you should stay on liquid diet and take acid-lowering tablets to prevent a stomach ulcer.
To prevent clots in the legs, we advise that you keep the elastic stockings we give you and to take the heparin injections for few days after leaving the hospital. This is why perhaps none of our patients have had clots after this type of surgery so far.
Dr Bart Decadt gives his personal number to all his patients (this is in addition to the contact numbers of the bariatric nurse, dietitian and the ward) so that they might reach him without delay in case of emergency.
Do I need to take vitamins after the surgery?
Although there is less risk of nutritional complications because of absence of malabsorption, we recommend that you take multivitamin (including 3-monthly injections of vitamin B12) on long-term basis and to have blood tests every year to check on these.
Will I regain weight?
The long-term results of this operation at 5 years and 10 years are still not available, particularly with regard to the rate of weight regain. Although this operation is not reversible, it is likely that some patients will stretch their stomach over time and therefore increase its capacity for food and calorie intake with subsequent weight regain. It is essential therefore to adopt a new life style and carry it on for a durable weight loss.
Bart Decadt
Consultant Laparoscopic Bariatric
& Upper GI Surgeon











Contact Private Secretary (Barbara Dawson)
Telephone 0161 440 9997 Fax 0161 440 8818 Mobile 07802 445558




CALCULATE YOUR BMI
THE PATIENT JOURNEY

All Enquiries
0161 440 9997




























request a quote
to request a quote or a call to discuss your surgical needs





to go to the NBSR website


“I enjoy attending the monthly support group sessions where I am helped by others who have experienced weight loss surgery..”





MBS (Manchester Bariatric Services)
